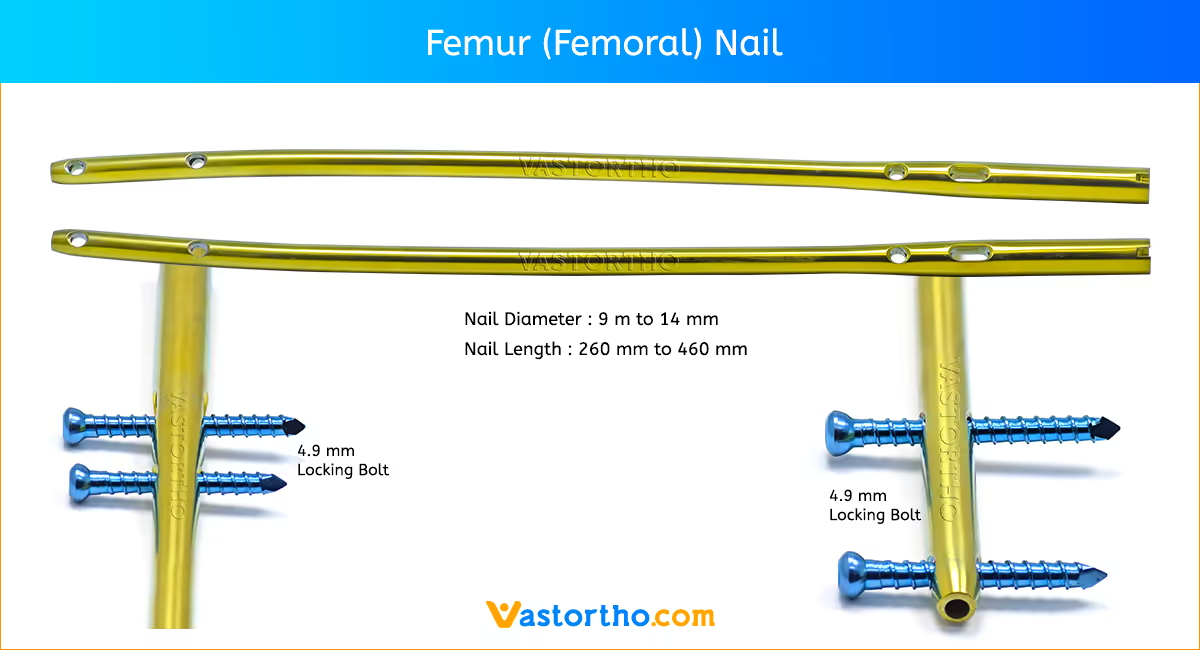
The Femur (Femoral) Nail is designed for varied use. A single nail can be used for both right and left standard interlocking or recon procedures. The femoral nail is available in the most commonly used sizes. These nails range in diameters from 9 mmm to 14 mm and lengths from 260 mm to 460 mm.
Preoperative Planning
Proper preoperative planning is essential to successful interlocking or recon nailing of the femur. To determine the appropriate nail size, an ossimeter, roentgenogram templates, and an x-ray film of the unaffected extremity are necessary for determining canal size at the isthmus and for measuring the length of the femur to aid in determining nail length. The Nail Length Gauge or Guide Wires, available in diameters from 10mm- 17mm, can be used as alternate techniques to determine nail diameter and length.
The proper length of Femur (Femoral) Nail should extend from the tip of the greater trochanter to the epiphyseal scar. The diameter of the femoral nail should match the isthmus in the lateral x-ray projection. The surgeon should review the x-ray to assure that there are no unusual anatomic variations.
Patient Positioning and Radiographic Control
The patient may be placed in either the supine or the lateral decubitus position.
In multiple trauma patients, the supine position may be used for easier access to the airways as well as to facilitate the treatment of other injuries. The supine position also facilitates fracture reduction and rotational alignment of the femur. The disadvantage to the supine position is that it impairs access to the tip of the greater trochanter for insertion of the nail. It is essential to obtain excellent A/P and lateral images of the femoral head and neck prior to beginning the surgery regardless of which patient position is used.
The use of image intensification or other x-ray imaging is required. The image intensifier should be steriledraped and may be positioned from either the contralateral or ipsilateral side of the operating table. Confirm visualization of the hip as well as
the shaft of the femur using image intensification before prepping and draping. Bend the patient’s torso away from the affected extremity to improve access to the greater trochanter. If access to the greater trochanter is still inadequate, adduct the affected leg. However, to achieve proper alignment of the fracture, this adducted position must be corrected prior to insertion of the nail.
Incision and Exposure
Begin the skin incision 1cm proximal to the greater trochanter and carry it proximally about 5cm in line with the gluteus maximus muscle. A larger incision may be desired for obese patients. Split the fascia of the gluteus maximus in line with its fibers. Identify the subfascial plane of the gluteus medius, and palpate the posterior tip of the greater trochanter. Retract the muscles to facilitate visualization of the piriformis fossa This may be difficult in the obese patient, especially if flexion causes the tip of the trochanter to lie against the ilium. Positioning techniques used to expose the tip of the trochanter include adduction of the leg and positioning of the patient’s torso away from the affected extremity.
Creating the Entry Portal
Locating the correct entry portal in the piriformis fossa is extremely important. For the interlocking procedure, place the Awl at the piriformis fossa and check its position with A/P and lateral views. For the recon procedure, place the Awl in the anterior portion of the piriformis fossa approximately 5mm anterior to the position you would choose when doing a standard femoral nailing . This will facilitate screw placement in the center of the femoral neck.
Check the position of the awl with both A/P and lateral images before creating the portal. On the A/P image, the awl should lie at the base of the femoral neck adjacent to the greater trochanter. On the lateral view, it should be oriented just posterior to the center of the femoral neck. When the correct position is achieved, rotate the Awl to create the entry portal for the Ball-Tip Guide Wire. If using the Long Cannulated Awl, the 2.5 mm Ball-Tip Guide Wire can be inserted through the Awl.
An alternative method is to insert a 3 mm Steinmann Pin into the piriformis fossa while checking the position with A/P and lateral image intensification. The Steinmann Pin must lie at the base of the femoral neck just medial to the greater trochanter on the A/P view, and oriented just posterior to the center of the femoral neck on the lateral view. Seat the Steinmann Pin well into the proximal femur and use the optional 9 mm Trochanteric Reamer to create the entry portal.
Guide Wire Replacement and Reaming
Attach the 2.5 mm Ball-Tip Guide Wire to the Wire-Grip T-Handle and tighten. To aid in manipulation, bend the tip of the Guide Wire at about a 10˚ angle 5cm from the end. Insert the Guide Wire through the entry hole and manipulate it down the proximal femur. At the fracture site, manipulate the Guide Wire under C-arm control. Once in the distal canal, pass the wire to its final position in the epiphyseal scar. If reduction of the abducted and flexed hip is difficult, place pressure on the anterior aspect of the proximal fragment either with the hand or directly with an instrument. The Reduction Finger can be used to assist in femoral fracture reduction. To use the Reduction Finger, advance the Ball-Tip Guide Wire and ream the proximal segment. Pass the Reduction Finger over the Ball-Tip Guide Wire. Manipulate the fracture externally While using the Reduction Finger internally to aid in fracture reduction. Once the Ball-Tip Guide Wire has passed through the fracture site, the Ball-Tip Guide Wire is advanced to epiphyseal scar. If the Ball-Tip Guide Wire can not advance through the fracture site, the ball tip of the Guide Wire should be bent
slightly and then reinserted to aid in internal reduction.
Determine the proper nail length by placing a second guide wire of equal length at the greater trochanter. The length of the wire that is not overlapping is the correct nail length. The 50cm Ruler or ossimeter may be used for an accurate measurement. Another way to measure the length is to use the C-arm to position the 0 mark on the metal ruler at the tip of the trochanter. Then read the correct length at the epiphyseal scar directly off the metal ruler. Alternatively, the IM Nail Length Gauge can be used to measure the appropriate Nail length through measurement of one 100cm Guide Wire. To use, place a 100cm Ball-Tip Guide Wire down the medullary canal. Slide the IM Nail Length Gauge over the Guide Wire, ensuring that the distal portion of the gauge is resting on the piriformis fossa in order to determine correct nail length. Nail length is determined by noting the location of the remaining Guide Wire and reading the Nail Length Gauge at that particular location. If the length indicated is between two available nail sizes, it is recommended that the shorter Femur (Femoral) Nail be chosen.
Remove the Wire-Grip T-Handle, and place a intramedullary reamer over the guide wire. The Intramedullary Reaming System is a system of one-piece reamers ranging in size from 7 mm diameter to 20 mm diameter in half millimeter increments. Each reamer is composed of a fluted reamer head, a shaft and a quick-connect drive end. The quick-connect end can be connected to a manual or powered driver. The width of the isthmus of the medullary canal is determined by preoperative x-ray examination. The instrument with the smallest possible diameter is used for initial reaming into the medullary canal. Reamers with a diameter of 5 mm to 7.5 mm use a 2.5 mm Ball-Tip Guide Wire while reamers with a diameter of 8 mm to 20 mm use a 3.0 mm Ball-Tip Guide Wire. As reaming continues, the reamer size should be increased by 0.5 mm or 1.0 mm increments until an opening of the desired size is obtained.
Femur (Femoral) Nail Insertion
Select the appropriate sized Femur (Femoral) Nail. Attach the selected nail to the appropriate left or right Femoral Proximal Targeting Guide. Insert the Femoral Locking Bolt through the barrel of the Proximal Targeting Guide. Using the thumb or finger to apply a steady downward pressure on the Locking Bolt, hand-tighten the Locking Bolt into the proximal end of the nail. Use the Pin Wrench to ensure that the locking mechanism is tightened securely. A keyway in the proximal end of the nail will help ensure proper alignment of the Guide and nail. The Lock Washer mechanism will prevent the Locking Bolt from loosening during the insertion of the nail. Tighten until the Lock Washer is flattened between the Guide and the Locking Bolt.
Interlocking Application
Verify proper alignment of the construct by inserting the 5mm Femoral Drill Bushing into the 8mm Femoral Screw Bushing. Insert the two nested bushings through the interlocking hole. Insert the 5mm Drill into the bushing and through the interlocking hole. When the device is properly aligned, the drill will pass through the proximal hole of the nail and will not contact the nail. Place the selected nail over the Ball-Tip Guide Wire and into the femur. Do not strike the guide directly to seat the nail. Screw the Threaded Driver or the Slaphammer into the back end of the Locking Bolt or onto the offset threaded drive. Begin seating the nail using gentle impaction. The Slotted Mallet can be used with the Threaded Driver to make slight upward adjustments in depth. While impacting the nail, use the Femoral Proximal Guide to maintain the proper rotation during impaction. Use caution when crossing the fracture site. Visualize the fracture in two planes with image intensification to assure proper passage of the nail into the distal fragment. Reduce the force of impaction as the proximal end of the nail approaches the greater trochanter.
Recon Application
When performing the recon procedure, slide a 14 in. Steinmann Pin percutaneously along the anterior aspect of the trochanter, parallel to the femoral neck. Verify pin placement with the C-arm. This will help to identify the anteversion of the neck. During the insertion, the Femoral Proximal Guide must remain parallel to this pin to ensure proper anteversion for the locking screws. If excessive resistance is encountered during nail driving, remove the Femur (Femoral) Nail and check the size of both the reamer and the nail. Once proper sizing has been confirmed, the surgeon may choose to over ream the canal or select a smaller size nail. Continue to seat the nail until it is flush with the trochanter. When the nail is fully seated, REMOVE THE GUIDE WIRE so that it does not get trapped in the bone. Remember, it might be concealed inside the driver or Slaphammer. Reassess the integrity of the Locking Bolt – Nail connection and re-tighten with the Pin Wrench if necessary.
Verify proper alignment by inserting the 3.2mm Femoral Pin/Drill Bushing into the 5mm Femoral Drill Bushing; then insert these two nested bushings into the 8mm Femoral Screw Bushing. Place the three nested guide bushings through one of the recon holes in the Femoral Proximal Guide. Insert the 3.2mm, 14in. Steinmann Pin through the inner bushing. When the device is properly aligned, the Steinmann Pin will pass through the proximal hole of the nail and will not contact the nail.
Proximal Locking
Screw the 5mm Femoral Drill Bushing, into the 8mm Femoral Screw Bushing, and insert them into the Femoral Proximal Guide. Insert the 5mm Femoral Drill, into the assembled bushings and drill until the medial femoral cortex is penetrated. Remove the 5mm Femoral Drill Bushing, leaving the 8mm Femoral Screw Bushing in place. Use the Proximal Screw Depth Gauge to determine screw length. Use the T-Handle Screwdriver to insert the appropriate length screw, to the correct reference line on the T-Handle Screwdriver. Use the C-arm to check the position of the screw and tighten it appropriately. Remove the screwdriver and the 8mm Femoral Screw Bushing. Take A/P and lateral C-arm views to check for correct positioning. If using a second Proximal screw, repeat the previous technique. Disengage the Locking Bolt from the nail using the Pin Wrench.
For Recon Application
Correct rotation of the Femur (Femoral) Nail is imperative for retrograde insertion of the two screws through the nail and into the femur. Be sure that the nail is inserted to the correct depth to allow placement of both screws with the correct anteversion. Screw the 3.2mm Proximal Pin/Drill Bushing, into the 5mm Femoral Drill Bushing. Screw this construct into the 8mm Femoral Screw Bushing, and insert the assembled three bushings into the inferior recon hole of the Femoral Proximal Guide to the level of the skin. Make an incision in the skin and fascia at this point and continue to insert the bushings until contact is made with the lateral femoral cortex. Drill a 14in. Steinmann Pin into the femoral head to the required level to achieve fracture fragment stability, without penetrating the femoral head cortex. Verify the proper position and anteversion of the pin with A/P and lateral C-arm views. Avoid excessive twisting or torquing of the Femoral Guide to ensure proper targeting. If the position is not correct, remove the pin and adjust the nail rotation and/or nail depth. Verify the new pin placement with the C-arm.
Assemble the second set of three bushings in the same fashion and place them into the superior hole of the Femoral Proximal Guide. Drill the second 14in. Steinmann Pin in to the bone and verify its position with the C-arm. If the position is unacceptable, remove both Steinmann Pins and reposition the nail. If the correct position is obtained, remove the Threaded Driver or Slaphammer. Also remove the inferior Steinmann Pin and the 3.2mm Proximal Pin/Drill Bushing. Insert the 5mm Femoral Drill, into the 5mm Femoral Drill Bushing. Drill the inferior proximal screw hole while monitoring image intensification to prevent penetration of the femoral head. Read the appropriate screw length directly from the calibrated Femoral Drill. Remove the 5mm Drill and Femoral Drill Bushing. Insert the Recon Screw Counterbore through the outer 8mm Femoral Screw Bushing and counterbore. The blunt end of the Counterbore serves as a stop.
Screw length may alternatively be measured using the Proximal Screw Depth Gauge. Select a screw equal to the measured length to avoid penetration of the joint. Another gauge that can be used to measure screw length is the Cannulated Depth Gauge. Slide the Cannulated Depth Gauge over the Steinmann Pin, i.e., the inferior of the two Steinmann Pins if two pins are used, until the gauge contacts the lateral aspect of the femur. Assess that the gauge is seated against the bone using the C-arm. Read and record the length of the Steinmann Pin from the calibrated depth gauge. Remove the counterbore using the T-Handle Screwdriver, insert the appropriate length 5.5mm Partially Threaded Recon Screw through the outer bushing to the level of the correct reference line on the T-Handle Screwdriver. Use the C-arm to ensure proper seating of the locking screw well within the femoral head. Tighten it appropriately.
The first screw should lie in the inferior neck to allow room for the second screw to be placed. This may be difficult in small patients or in patients with varus hips. Be certain to seat the inferior screw tightly against the medial cortex to prevent varus deformity and to allow for placement of the proximal screw. Remove the T-Handle Screwdriver and the Femoral Bushing. Take A/P and lateral C-arm views to check for correct positioning. Repeat the same procedures for insertion of the superior
locking screw. Again, observe A/P and lateral C-arm views to ensure proper seating within the femoral head and neck. Using the Pin Wrench, loosen and remove the Locking Bolt and Femoral Proximal Guide.
Distal Locking
The distal locking screws may be inserted with a freehand technique using the Freehand Targeting Device. Insert an appropriate size Trocar into the Freehand Targeting Device. Finger tighten the set screw. Choose the appropriate locking hole based on the need for dynamization. The superior locking hole on Femur (Femoral) Nail is used for static locking, while the distal locking hole is used for dynamic locking. If static locking is preferred, but there is a potential need for later dynamization, insert screws in both locking holes. The locking screw in the static hole can then be removed to achieve later dynamization. For success with this technique, proper placement of the lateral x-ray beam is critical. Position the C-arm so the locking hole of the nail appears perfectly round on the monitor.
When this is achieved, bring the tip of the Trocar to the skin and use the C-arm to center it over the hole. Make a lateral stab wound opposite the appropriate locking hole, and dissect down to bone. Bring the tip of the Trocar to the bone and center it over the locking hole using the C-arm. Align the Trocar with the axis of the x-ray beam. Drive the Trocar into the bone and across the hole in the nail in line with the lateral x-ray beam, but do not penetrate the medial cortex. Remove the Targeting Device by loosening the set screw. Verify Trocar placement in both the A/P and lateral planes. After it has been correctly placed, remove the Trocar. The path of the Trocar in the bone acts as a pilot hole for the appropriate size drill. Attach the appropriate drill (same size as the Trocar) to the Freehand Targeting Device. Insert the drill into the pilot hole made by the Trocar. Before drilling through the medial cortex, check the A/P and lateral C-arm image to assure that the drill is in the hole in the nail. Then drill through the medial cortex.
Remove the drill and insert the Distal Screw Depth Gauge. The length of the screw is determined by reading it directly off the Distal Screw Depth Gauge. Select an appropriate length screw to ensure adequate engagement of the medial cortex. Insert the appropriate size Screw using the Screwdriver.If desired, insert the second screw in the second locking hole of the nail in an identical manner. Check the position of both screws with the C-arm in the A/P and lateral planes. Bushings are available that can be used with the Freehand Targeting Device. A separate radiolucent Bushing Insert is available to aid in targeting.