2.5 mm Screws Length
8mm, 10mm, 12mm, 14mm, 16mm, 18mm, 20mm, 22mm, 24mm, 26mm, 28mm and 30mm.
3 mm Screws Length
8mm, 10mm, 12mm, 14mm, 16mm, 18mm, 20mm, 22mm, 24mm, 26mm, 28mm and 30mm.
3.5 mm Screws Length
8mm, 10mm, 12mm, 14mm, 16mm, 18mm, 20mm, 22mm, 24mm, 26mm, 28mm, 30mm, 32mm, 34mm, 36mm, 38mm, 40mm, 42mm, 44mm, 46mm, 48mm, 50mm, 55mm, 60mm, 65mm, 70mm, 75mm and 80mm.
4.5 mm Screws Length
8mm, 10mm, 12mm, 14mm, 16mm, 18mm, 20mm, 22mm, 24mm, 26mm, 28mm, 30mm, 32mm, 34mm, 36mm, 38mm, 40mm, 42mm, 44mm, 46mm, 48mm, 50mm, 55mm, 60mm, 65mm, 70mm, 75mm and 80mm.
5.5 mm Screws Length
12mm, 14mm, 16mm, 18mm, 20mm, 22mm, 24mm, 26mm, 28mm, 30mm, 32mm, 34mm, 36mm, 38mm, 40mm, 42mm, 44mm, 46mm, 48mm, 50mm, 55mm, 60mm, 65mm, 70mm, 75mm, 80mm, 85mm, 90mm, 95mm, 100mm, 105mm, 110mm, 115mm and 120mm.
6.5 mm Screws Length
12mm, 14mm, 16mm, 18mm, 20mm, 22mm, 24mm, 26mm, 28mm, 30mm, 32mm, 34mm, 36mm, 38mm, 40mm, 42mm, 44mm, 46mm, 48mm, 50mm, 55mm, 60mm, 65mm, 70mm, 75mm, 80mm, 85mm, 90mm, 95mm, 100mm, 105mm, 110mm, 115mm and 120mm.
 https://www.vastortho.com/wp-content/uploads/2.5-mm-Herbert-Screws.jpg
700
1200
VastOrtho
https://www.vastortho.com/wp-content/uploads/Vast-Ortho-Logo-for-website.png
VastOrtho2020-01-05 12:54:362023-07-22 17:43:502.5 mm Herbert Screw
https://www.vastortho.com/wp-content/uploads/2.5-mm-Herbert-Screws.jpg
700
1200
VastOrtho
https://www.vastortho.com/wp-content/uploads/Vast-Ortho-Logo-for-website.png
VastOrtho2020-01-05 12:54:362023-07-22 17:43:502.5 mm Herbert Screw https://www.vastortho.com/wp-content/uploads/3-mm-Herbert-Screws.jpg
700
1200
VastOrtho
https://www.vastortho.com/wp-content/uploads/Vast-Ortho-Logo-for-website.png
VastOrtho2020-01-04 11:36:492023-07-22 17:44:273 mm Herbert Screw
https://www.vastortho.com/wp-content/uploads/3-mm-Herbert-Screws.jpg
700
1200
VastOrtho
https://www.vastortho.com/wp-content/uploads/Vast-Ortho-Logo-for-website.png
VastOrtho2020-01-04 11:36:492023-07-22 17:44:273 mm Herbert Screw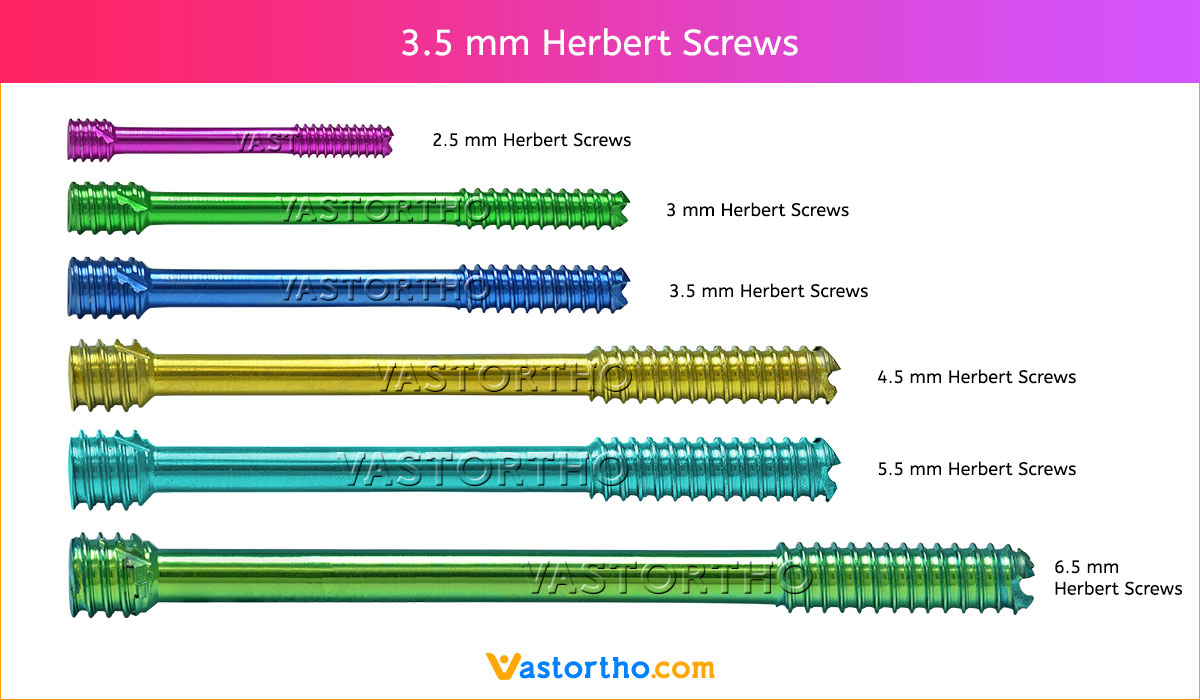 https://www.vastortho.com/wp-content/uploads/3.5-mm-Herbert-Screws.jpg
700
1200
VastOrtho
https://www.vastortho.com/wp-content/uploads/Vast-Ortho-Logo-for-website.png
VastOrtho2020-01-03 11:51:562023-07-22 17:44:383.5 mm Herbert Screw
https://www.vastortho.com/wp-content/uploads/3.5-mm-Herbert-Screws.jpg
700
1200
VastOrtho
https://www.vastortho.com/wp-content/uploads/Vast-Ortho-Logo-for-website.png
VastOrtho2020-01-03 11:51:562023-07-22 17:44:383.5 mm Herbert Screw https://www.vastortho.com/wp-content/uploads/4.5-mm-Herbert-Screws.jpg
700
1200
VastOrtho
https://www.vastortho.com/wp-content/uploads/Vast-Ortho-Logo-for-website.png
VastOrtho2020-01-01 12:35:452023-07-22 17:44:524.5 mm Herbert Screw
https://www.vastortho.com/wp-content/uploads/4.5-mm-Herbert-Screws.jpg
700
1200
VastOrtho
https://www.vastortho.com/wp-content/uploads/Vast-Ortho-Logo-for-website.png
VastOrtho2020-01-01 12:35:452023-07-22 17:44:524.5 mm Herbert Screw https://www.vastortho.com/wp-content/uploads/5.5-mm-Herbert-Screws.jpg
700
1200
VastOrtho
https://www.vastortho.com/wp-content/uploads/Vast-Ortho-Logo-for-website.png
VastOrtho2020-01-01 12:30:052023-07-22 17:45:515.5 mm Herbert Screw
https://www.vastortho.com/wp-content/uploads/5.5-mm-Herbert-Screws.jpg
700
1200
VastOrtho
https://www.vastortho.com/wp-content/uploads/Vast-Ortho-Logo-for-website.png
VastOrtho2020-01-01 12:30:052023-07-22 17:45:515.5 mm Herbert Screw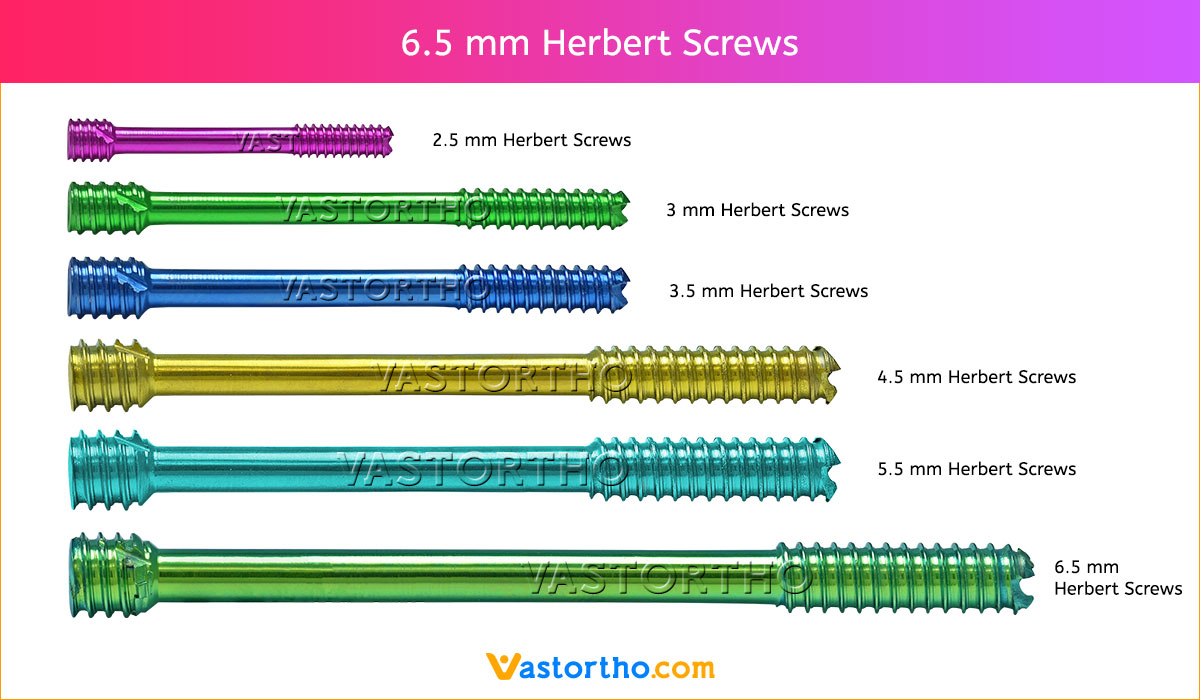 https://www.vastortho.com/wp-content/uploads/6.5-mm-Herbert-Screws.jpg
700
1200
VastOrtho
https://www.vastortho.com/wp-content/uploads/Vast-Ortho-Logo-for-website.png
VastOrtho2020-01-01 12:25:452023-07-22 17:46:056.5 mm Herbert Screw
https://www.vastortho.com/wp-content/uploads/6.5-mm-Herbert-Screws.jpg
700
1200
VastOrtho
https://www.vastortho.com/wp-content/uploads/Vast-Ortho-Logo-for-website.png
VastOrtho2020-01-01 12:25:452023-07-22 17:46:056.5 mm Herbert Screw

